By Bryan Groleau
COTA/L, CLT-LANA, WCC, LLE
Over the last decade, oncology surgeons have succeeded in reducing the frequency and severity of oncology related lymphedema through dramatic improvements in axillary treatment. The days of vast radical mastectomies are gone. For years surgeons have been removing fewer lymph nodes through sentinel lymph node dissection, and developing new procedures such as lymph node transplant and lymphovenous bypass, and are now exploring other microsurgeries to lessen the blow of lymphedema.1
Oncologists are even making referrals for compression earlier thanks to technological advancements such as bioimpedance spectroscopy devices that identify lymphedema as early as the subclinical latency stage, mitigating the effects of lymphedema and reducing the number of cases which progress to irreversible stages.2,3
Because oncology related lymphedema is being identified earlier, fewer patients are in need of extensive outpatient lymphedema treatment. Still, we’re seeing an unprecedented demand for certified lymphedema therapists (CLTs) and outpatient lymphedema treatment programs nationwide. One might question why we are seeing such exponential growth in lymphedema rehabilitation.
The answer: Phlebolymphedema.
Phlebolymphedema is the most common and, perhaps, least understood form of lymphedema, yet it is quite different from oncology-related lymphedema which practitioners came to understand years ago. Diagnosing lymphedema is largely dependent upon clinical presentation, but unlike vein disease which shows definitive clinical symptoms, typical characteristics of lymphedema do not manifest externally until its permanent, advanced stages.4,5,6
Thus, wound centers, along with vascular and podiatry clinics, are full of patients with unidentified phlebolymphedema. One of my goals as the national clinical educator for MediUSA is to spread awareness of this hidden disease and help practitioners learn to identify and effectively treat phlebolymphedema. When the lymphedema component goes unrecognized and adjunct treatments are not put into place, the patient’s comprehensive needs are not fully addressed.
Identification
Lymphedema is classified into two types: Primary, which derives from developmental abnormalities or genetic mutations, and Secondary, which results from external factors that cause disruptions in the lymphatic system such as surgical interventions, radiation and/or infection. Secondary lymphedema is most commonly associated with oncology lymphedema in which the cancer treatment through surgery and radiation leads to lymph node removal and damaged tissue causing blockages in lymph flow.
However, mechanical insufficiency is only one form of secondary lymphedema; in actuality, there are two forms. Dynamic insufficiency, on the other hand, includes phlebolymphedema which occurs when the lymphatic load exceeds the maximum transport capacity.7
When either form of secondary lymphedema occurs, protein accumulation in the tissue triggers an inflammatory response leading to skin changes characteristic of lymphedema such as hyperkeratosis and papillomatosis and will also present with a positive Kaposi Stemmer sign, a pathognomonic indication of lymphedema.
Early identification is a crucial step toward successful management and the prevention of advanced stages of lymphatic disease. It may seem easy enough to understand how reflux associated with vein disease can lead to lymphatic overload; however, knowing the specific etiology of a patient’s vein disease may give insight to the presentations of lymphedema.
70% of chronic venous insufficiency is due to weakening of the bicuspid valves (primary CVI), leading to stasis in the interstitial tissue. The other 30% is due to venous obstruction (secondary CVI).8 Whenever reflux occurs, the lymphatic system must work above its normal load to achieve homeostasis. Eventually, if the amount of fluid exceeds the lymphatic maximum transport capacity, edema will occur.9
For this reason, phlebolymphedema becomes identifiable when edema is evident. What is popularly referred to as venous edema could also be identified as an early Stage 0 or Stage 1 lymphedema due to a coexisting malfunction in the lymphatic vessels. Stage 0 Lymphedema has no clinical presentation, and Stage 1 Lymphedema involves visible edema that goes away with elevation.
Both are reversible if identified early and appropriate interventions are put into place. Unfortunately, phlebolymphedema often goes unnoticed until the clinical characteristics become more obvious in Stage 2, at which point the patient will require lifelong self-care maintenance.
Intervention
Traditional lymphedema therapy practices were developed with the oncology lymphedema patient in mind. Swelling caused by mechanical dysfunction to the lymphatic system is treated through Complete Decongestive Therapy (CDT) which focuses on moving lymph away from the affected lymph nodes. CDT performed by a CLT consists of Manual Lymph Drainage (MLD), compression therapy, remedial exercises, skin-care, and education in self-care. This standard protocol focuses on utilizing MLD to reroute congested lymph fluid across anastomoses toward alternate lymph nodes located opposite of the natural lymphatic pathway. Multilayer compression bandaging is then applied to the entire limb to promote lymph flow in that same MLD direction away from the affected lymph nodes. However, it is important to understand phlebolymphedema is not caused by mechanical dysfunction. The lymphatics are intact and therefore requires a different treatment approach.
In some instances, compression alone has been shown to reduce phlebolymphedema. For example, in wound care, some venous leg ulcers with coexisting lymphedema will heal when appropriate compression is applied without ever requiring a referral to a CLT.
Understanding the vascular and lymphatic pathology of phlebolymphedema and recognizing the various stages of this disease will help practitioners determine whether they can manage the patient’s swelling with compression or if a referral to a CLT is needed. Patients with more severe lymphedema will need to be referred to a certified lymphedema specialist who will not only provide appropriate compression solutions but also provide individualized treatment.
Treatment for advanced phlebolymphedema should consist of MLD, utilizing the normal medial pathway toward inguinal lymph nodes followed by compression to the knee. Phlebolymphedema derived from DVT may require full limb compression depending on location of the thrombosis. Not all CLTs share extensive knowledge of phlebolymphedema. Therefore, be sure to include relevant information regarding the patient’s vascular disease to help the lymphedema therapist determine the best course of action for the patient.
Important medical history to share with the CLT may include the following: patient’s CEAP classification (Comprehensive Classification System for Chronic Vein Disorders); location; status and treatments of a DVT with specific aspects of CDT indicated/contraindicated and/or requiring precautions; and information on ABI (ankle-brachial Index) and/or TBI (Toe-Brachial Index) with specified precautions with compression. Keeping an open line of communication with the CLT is recommended for continuity of care to assure the patient will receive the most effective plan of care for their individual needs.
Compression recommendations
The most appropriate compression product(s) for the phlebolymphedema patient are those which will not only stimulate lymph return and support the lymphatic system, but will simultaneously and effectively address the patient’s vein disease. Compression levels at 30-40mmHg or higher are recommended whenever possible for the phlebolymphedema patient, with 40-50mmHg being the most adequate level of compression due to dual-system failure. Compression levels should really only be reduced in the presence of moderate to severe PAD with ABI levels below 0.8.10

Primary phlebolymphedema (originating through weakened bicuspid valves in the veins) makes up the majority of cases and is generally very responsive to compression therapy. Often dramatic results can be seen within a single week. Compression to the knee is typically sufficient, with the exception of secondary phlebolymphedema (post-thrombotic), as swelling can oftentimes be present throughout the entire limb. Swelling above the knee could be a red flag indicating possible presence of other edema types. Practitioners should consider the patient’s comorbidities to determine whether precautionary steps are needed or if treatment is contraindicated. Because primary phlebolymphedema has the potential to reduce quickly, using adjustable compression wraps can expedite the treatment process by allowing compression to be readjusted as swelling reduces.
Circaid by MediUSA offers a complete line of inelastic adjustable compression garments designed with the specific indications for wound care and phlebolymphedema in mind. Every Circaid wrap features Velcro, allowing for instantly adjustable compression, while providing the gradient, dosage, and wall stability needed to effectively combat edema.11 This comprehensive product line includes both ready-to-wear and custom-fit compression ideal for venous, lymphatic and wound care applications.
The Juxtalite HD (heavy duty) wrap is an excellent option for the wound care setting and is covered by Medicare and many health insurances when prescribed for patients with an open wound. I recommend both the Circaid Juxtafit and Circaid reduction kit for treating more advanced stages of lymphedema.
In addition to allowing for adjustability, the Circaid Juxtalite, Juxtalite HD and Juxtafit are designed with Circaid’s patented built-in-pressure system™ (BPS™) which allows the patient to adjust the product to their prescribed compression range, such as 20-30mmHg or 30-40mmHg. All Circaid compression products offer the benefit of providing simplified ease of donning and doffing, to help patients self-manage their disease, which is especially important for geriatric patients who so-often struggle with applying appropriate compression.
Additionally, pneumatic compression devices can be of use for the phlebolymphedema patient but should not be used as a replacement for lymphedema therapy or in place of compression garments. Pneumatic compression should be an adjunct to therapy and only obtained after the appropriate maintenance compression products have been put in place.
Lymphedema pumps have been of some controversy among the lymphedema community for years and are oftentimes not recommended due to the pump’s inability to reroute lymph fluid to alternate unaffected areas. However, rerouting of lymph fluid is generally not required when considering the etiology of vein disease because the affected limb’s own inguinal lymph nodes can be utilized. For this reason, basic pneumatic compression like the Medi PCS Brio can be utilized without damage to the lymphatic system as it also addresses the venous components of circulation simultaneously.
Mixed Etiology
The complexity of phlebolymphedema is generally not stemmed from the vein disease itself but the comorbidities that come with a predominately geriatric patient population. Patients who develop CVI are generally elderly patients already experiencing degenerative repercussions of the natural aging process, and their venous health is often not prioritized until a wound is present.
For this reason, many patients with phlebolymphedema already have advanced lymphedema by the time they are referred to therapy and probably already have edema associated with comorbidities such as CHF, Kidney disease, hypertension, sleep apnea, and/or obesity. These comorbidities complicate treatment since the swelling is now of mixed etiology.
Practitioners must determine whether the patient will be able to tolerate the treatment plan to reduce the swelling and whether decongestive therapy is possible for the patient. Furthermore, elderly and/or obese patients will usually have a harder time completing self-care skills needed for lifelong maintenance of the edema, especially when it comes to donning/doffing compression.
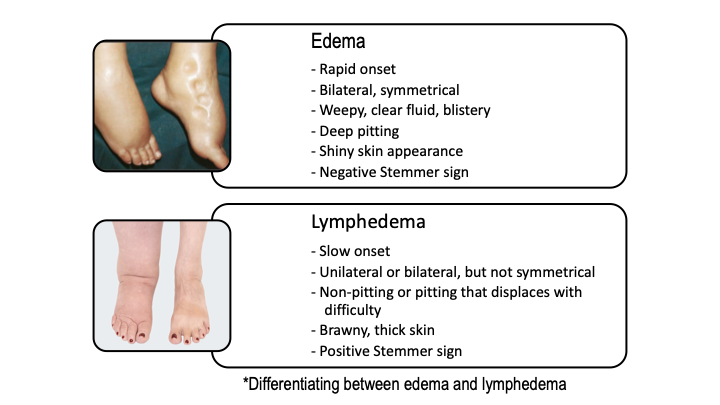
The following characteristics that can help differentiate phlebolymphedema from edema to determine the best course of action for your patient. (See attached comparative chart.)
All practitioners involved in the care of patients with vein disease, whether through cardiovascular health care, podiatry, wound care, or lymphedema therapy, should consider the lymphedema component of vein disease as early as possible. Identification can prevent a host of complications including venous leg ulcers, late stage lymphedema, inflammatory fibrotic conditions such as lipodermatosclerosis, and/or skin conditions such as hyperkeratosis and papillomatosis. Early identification of phlebolymphedema with proactive intervention has the power to prevent this disease from entering its permanent stages and will greatly improve patient care and quality of life. VTN
 Bryan Groleau, a national senior clinical education manager for mediUSA, specializes in lower extremity lymphedema and wounds. Since 2003, Bryan has treated all types of lymphedema in outpatient and home health settings, has initiated and managed multiple lymphedema and wound care programs, and has treated patients with Lymphatic Filariasis in Léogâne, Haiti, with medi for help.
Bryan Groleau, a national senior clinical education manager for mediUSA, specializes in lower extremity lymphedema and wounds. Since 2003, Bryan has treated all types of lymphedema in outpatient and home health settings, has initiated and managed multiple lymphedema and wound care programs, and has treated patients with Lymphatic Filariasis in Léogâne, Haiti, with medi for help.
References
- Brucker BD, Zeltzer A, Seidenstuecker K, Hendrickx B, Adriaenssens N, Hamdi M. Breast Cancer–Related Lymphedema. Plastic and Reconstructive Surgery. 2016;137(6):1673-1680. doi:10.1097/prs.0000000000002169.
- Pasket ED, Dean JA, Oliveri JM, Harrop JP. Cancer-Related Lymphedema Risk Factors, Diagnosis, Treatment, and Impact: A Review. Journal of Clinical Oncology. 2012, 30(30):3726-3733. doi: 10.1200/JCO.2012.41.8574
- Ridner, S.H., Dietrich, M.S., Cowher, M.S. et al. A Randomized Trial Evaluating Bioimpedance Spectroscopy Versus Tape Measurement for the Prevention of Lymphedema Following Treatment for Breast Cancer: Interim Analysis. Ann Surg Oncol 2019, 26: 3250–3259. doi: 10.1245/s10434-019-07344-5
- Rockson, S. Bioimpedance analysis in the assessment of lymphoedema diagnosis and management. J Lymphoedema 2007;2(1):44–8
- Farrow W. Phlebolymphedema–a common underdiagnosed and undertreated problem in the wound care clinic. J Am Col Certif Wound Spec. 2010;2(1):14-23.
- Bunke, N., Brown, K., & Bergan, J. Phlebolymphedema: Usually Unrecognized, Often Poorly Treated. Perspectives in Vascular Surgery and Endovascular Therapy 2009;21(2), 65–68. https://doi.org/10.1177/1531003509337155
- Lee BB. Phlebolymphedema: Neglected Outcome of Combined Venous and Lymphatic Insufficiency. Vasc Specialist Int. 2020;36(1):1-3. doi:10.5758/vsi.2020.36.1.1
- Patel SK, Surowiec SM. Venous Insufficiency. [Updated 2020 Feb 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430975/
- Piller, N. Phlebolymphoedema/chronic venous lymphatic insufficiency: an introduction to strategies for detection, differentiation and treatment. Phlebology. 2009;24(2), 51–55. https://doi.org/10.1258/phleb.2009.009003
- de Carvalho MR, de Andrade IS, de Abreu AM, Leite Ribeiro AP, Peixoto BU, de Oliveira BG. All about compression: A literature review. J Vasc Nurs. 2016;34(2):47-53. doi:10.1016/j.jvn.2015.12.005
- Groleau B. Essentials of Compression—Lymphedema Therapist: Consider Gradient, Dosage, Adjustability, Wall Stability. Vein Therapy News. 2020;13(3):1,20-21,27.
